Trigger Finger
This is a common condition whereby a finger is initially difficult to tuck into a fist. If one does curl it in, it will then get ‘stuck’ and refuse to easily straighten out. The ‘trigger’ refers to a sudden release of the finger on continued effort whereupon it springs/ pops straight again. This is often painful, and sometimes must be performed manually by the patient pulling the fingertip out with their opposite hand.
The lack of free gliding has a mechanical basis. Our fingers are moved by ropes (tendons) which run in a pulley system (sheath), not unlike cable-driven bicycle brakes. All gliding surfaces are lined by a lubricating layer (synovium), and this can thicken up from a variety of causes. The commonest are degenerative (wear and tear), rheumatoid and diabetes, the 2 latter often associated with multiple finger involvement.
Trigger fingers are commoner in women, and tend to be associated with Carpal Tunnel Syndrome, deQuervain’s (another form of tenosynovitis affecting the back of the thumb) and Tennis Elbow. Sometimes a tender lump in the palm denotes the site where the tendon is getting trapped or having difficulty negotiating its sheath.
Treatment is initiated in a stepwise escalating manner, as in many chronic hand conditions. Initially one may try ‘gliding exercises’ delivered through a Hand Therapist. If this does not help, or the condition is too far advanced, a Corticosteroid injection into the trigger site under local anaesthetic in Clinic itself is often successful. The effect is usually temporary though, and a proportion of patients will eventually need surgery. This is usually performed under local anaesthetic as a short day-case. For certain digits, this can be done without opening the skin using a thick needle as an office procedure.
Instead of this blind percutaneous approach, Mr Agarwal prefers doing the operation under magnification through a small 2cm cut in the skin in theatre. Sterility is guaranteed and the delicate clockwork of the hand can be clearly seen, allowing proper full release. Rapid recovery and a permanent cure of the trigger are to be expected with good post-operative physiotherapy. The downtime off work and driving is variable, averaging a week. Mr Agarwal can tailor the treatment options to your specific needs.
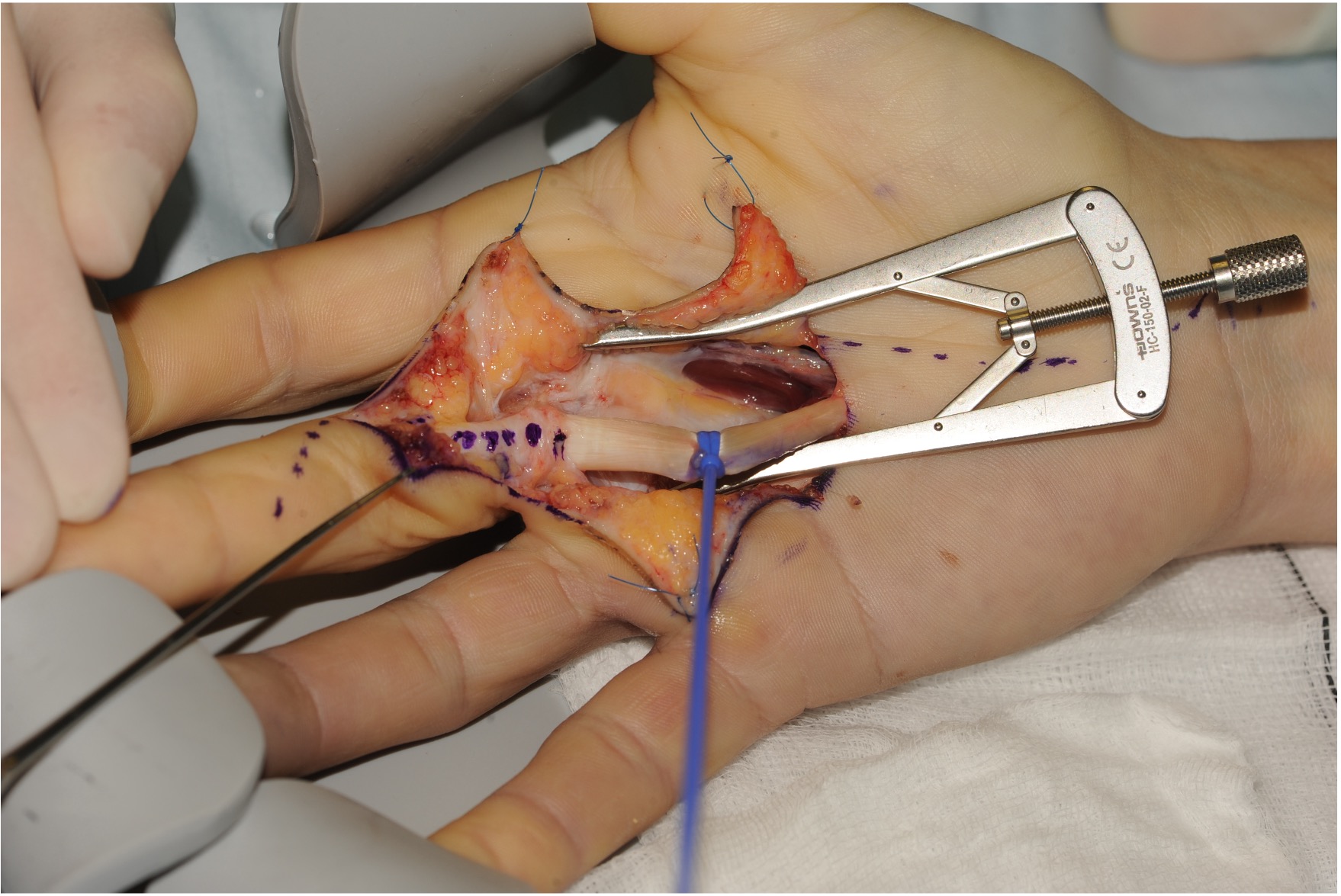
Rarely in stiff, puffy rheumatoid fingers, a much longer incision to fully debulk the thickened synovium (formal Synovectomy Surgery) may be required (Fig). Naturally, this needs much more intense Physiotherapy and takes longer to recover from.